Tsutomu Fujita, MD.
Sapporo Cardiovascular Clinic, Japan
Yutaka Tadano, MD.
Sapporo Cardiovascular Clinic, Japan
Shoichi Kuramitsu, MD.
Sapporo Cardiovascular Clinic, Japan
We were honored to welcome participants from all over the world, who joined us for engaging and advancing CTO-PCI.
On behalf of the CTO & CHIP JAPAN Organizers, we extend our heartfelt thanks to all faculty, participants, and partners who contributed to the success of this meaningful educational event.
Your insights, expertise, and shared passion are what continue to drive innovation in complex PCI worldwide.

Tsutomu Fujita, MD.
Sapporo Cardiovascular Clinic, Japan
Yutaka Tadano, MD.
Sapporo Cardiovascular Clinic, Japan
Shoichi Kuramitsu, MD.
Sapporo Cardiovascular Clinic, Japan
The official website is now live! The inaugural session is scheduled for Saturday, April 12, 2025, from 10:00 to 14:30 (JST). Please check the website for viewing details.https://t.co/OtxCLd4xiq pic.twitter.com/WwYfhO3PSb
— CTO&CHIP JAPAN (@cto_chip_japan) January 24, 2025
Since the world's first percutaneous coronary intervention (PCI) was performed in September 1977, advancements in medical devices have been paralleled by significant progress in the skills of interventional cardiologists. PCI rapidly gained traction as a minimally invasive therapeutic option for patients who could not be effectively managed with pharmacological therapy but did not require coronary artery bypass grafting. It soon became the gold standard for treating ischemic heart disease.
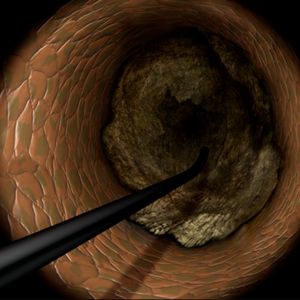
From the era of Plain Old Balloon Angioplasty (POBA) to bare-metal stents (BMS) and subsequently drug-eluting stents (DES), PCI has evolved to become the primary treatment modality for increasingly complex lesions. Among these, chronic total occlusions (CTOs) were considered the "last frontier" of PCI, prompting the development of techniques to guide wires through completely occluded lesions.
In Japan, PCI evolved under the unique circumstances of a universal healthcare system, where fewer restrictions on time and cost allowed for more flexible approaches compared to Western countries. From the late 1990s to the early 2000s, innovative techniques such as the parallel wire technique and IVUS-guided wiring emerged in Japan. However, despite the implementation of these methods, initial technical success rates for CTO-PCI remained around 80%.
In the mid-to-late 2000s, the retrograde approach was introduced, leveraging collateral channels for wire crossing, significantly improving the success rates of CTO-PCI. This technique gained widespread attention due to the expertise of Japanese operators, elevating the global recognition of Japan's contributions. However, the use of delicate collateral channels posed challenges, particularly for less experienced interventional cardiologists, leading to complications such as perforations. Consequently, enthusiasm for CTO-PCI waned in Western countries, where its perceived lack of reproducibility kept it relegated to the realm of mastery-level procedures.
A new wave of technological innovation emerged in the late 2010s with the introduction of the 3D wiring technique. Developed by Dr. Atsunori Okamura of Sakurabashi Watanabe Hospital, this method enabled three-dimensional visualization of wires within occluded lesions, allowing precise manipulation by observing the movement of the wire tip in three dimensions. This rational approach transitioned CTO-PCI wiring from a skill dependent on tactile sensation to one guided by scientific observation.
The 3D wiring technique was further refined by expert operators across Japan, eventually establishing Tip Detection Antegrade Dissection Re-entry (TD-ADR) as a new standard in CTO-PCI. TD-ADR reignited global interest in CTO-PCI by providing a more systematic and reproducible methodology. More recently, HydroDynamic Contrast Recanalization (HDR) has emerged as a technique for performing antegrade CTO-PCI, leveraging the synergistic use of contrast microinjections and polymer-jacketed wires to further expand the technical options available for CTO-PCI.
Compared to conventional approaches to CTO-PCI, the emergence of TD-ADR and HDR has significantly reduced costs, procedure times, and complication risks. These advancements inspire confidence that CTO-PCI, often referred to as the "last frontier" of PCI, could become a fundamental treatment for totally occluded lesions.
To accelerate research and development in CTO-PCI, CTO&CHIP courses have been held worldwide, fostering collaboration among interventional cardiologists. In line with this trend, we have established "CTO&CHIP JAPAN," a course uniquely tailored to Japan. This course aims to pursue rational and reproducible CTO-PCI techniques without adhering solely to Japanese methods, aligning with global standards.
The official language of the course will be English, allowing for in-depth discussions with global leaders in CTO-PCI and promoting further advancements in treatment. For the first session, Dr. Tsutomu Fujita and Dr. Atsunori Okamura will perform live demonstrations, with global leaders participating online. We invite all healthcare professionals to join us in this new endeavor, exploring the "last frontier" of PCI pioneered by Andreas Gruentzig 50 years ago.
Tsutomu Fujita, MD.
Chair of CTO&CHIP JAPAN